
Read this in three ways
- Skim in 2 minutes
Use the jump cards and the takeaway boxes at the end of each section.
- Use it today
Open the field-guide tools, then bring the appointment script, flare card, or tracker to your next real-world decision.
- Read deeply
Follow the full guide with the evidence labels: strong, moderate, community pattern, and anecdotal.
How this was written
One term matters before we go further: axial spondyloarthritis, or axSpA. Ankylosing spondylitis is often used for radiographic axSpA, where damage is visible on plain X-ray; non-radiographic axSpA can produce the same inflammatory pattern before X-ray changes are obvious. That matters for people with normal X-rays, women, HLA-B27-negative patients, and anyone being told the scan has ended the conversation[12].
Patient communities for AS are some of the most generous places on the internet. People share things there they would never tell a doctor — partly because nobody asked, partly because the doctor doesn't have twenty minutes to listen, partly because only another person living with this disease can understand the answer. Those forums hold wisdom you cannot get from a clinical trial: what mornings actually feel like, what a biologic switch looks like over months, what a flare does to a marriage.
But community wisdom and clinical evidence are not the same thing, and pretending they are is how people get hurt. So every lesson here is graded — labelled by how strong the evidence actually is, from guideline-backed fact to one person's experiment. Read the key, then read everything against it.
- StrongGuidelines, randomized trials, or meta-analyses.
- ModerateGood observational data or large patient surveys.
- Community patternWidely reported across forums; limited formal evidence.
- AnecdotalIndividual reports — try carefully, prove on yourself.
The diagnostic odyssey
This story is so common the literature treats it as a syndrome. Diagnostic delay in axSpA pools to a mean of roughly 6.7 years across studies[2]. In a survey of 235 US patients, 33% took ten years or more; another 30% took two to nine[1]. Women — 74% of respondents — were far more often misdiagnosed with fibromyalgia (~21% vs ~7% for men) and “psychosomatic” disorders (~41% vs ~23%)[1].
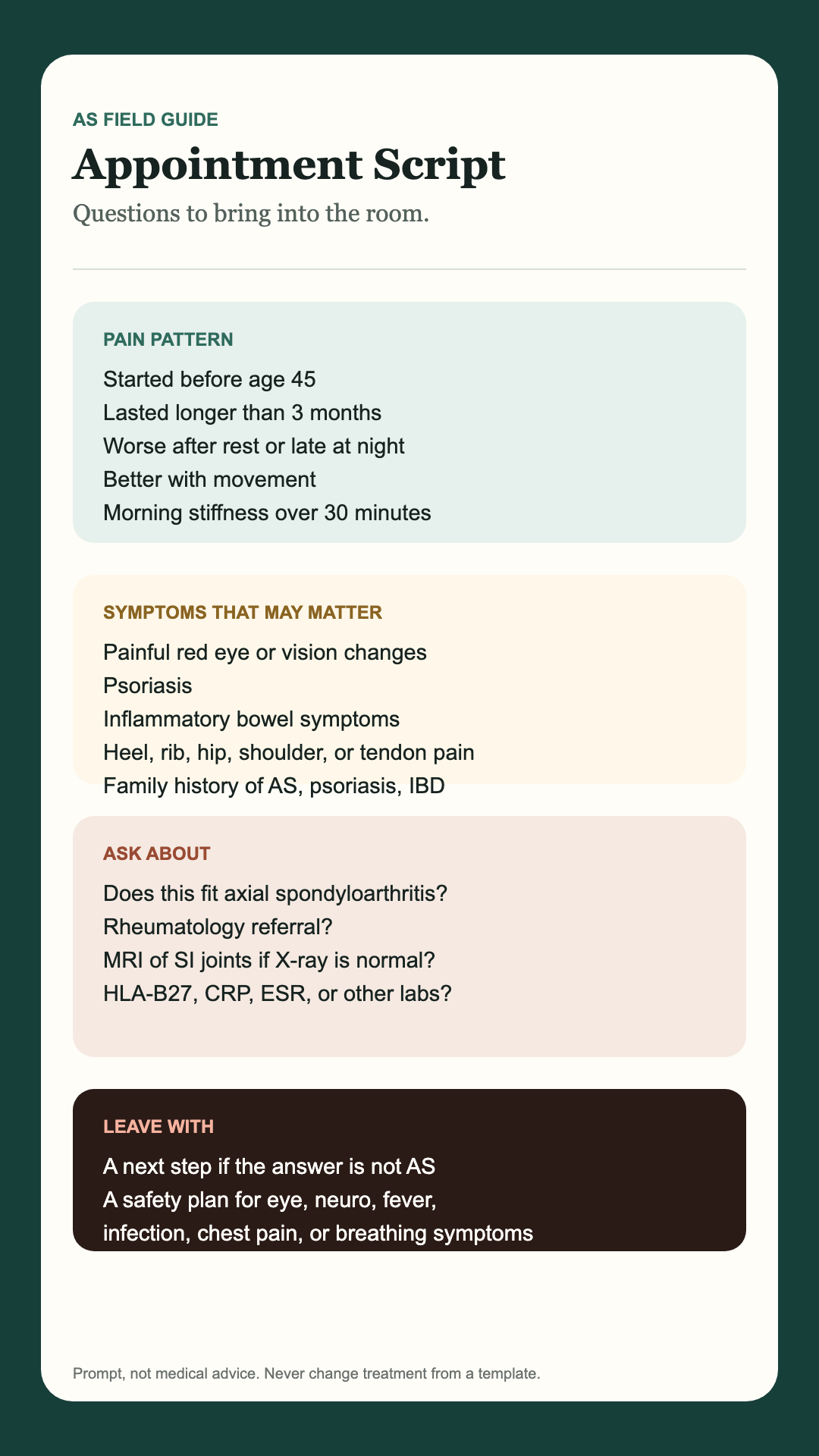
- Strong evidenceAsk the MRI question. A normal X-ray does not rule out axial spondyloarthritis. In early or non-radiographic disease, MRI of the sacroiliac joints may be needed, and a rheumatologist should interpret the full pattern, not one image in isolation[12]. Ask whether an MRI of the SI joints, including fluid-sensitive/STIR sequences, is appropriate.
- Strong evidenceKnow the inflammatory fingerprint. Write it down and bring it: onset before 45, lasting 3+ months, worse with rest, better with movement, morning stiffness over 30 minutes[11]. That pattern is what gets a referral.
- Moderate evidenceHLA-B27 is a clue, not a verdict. Negative doesn't rule AS out and positive doesn't confirm it — but the result, plus the fingerprint, gets you taken seriously by the next clinician[12].
- Community patternThe eye is a clue, not an eye problem. A painful, light-sensitive red eye (uveitis) is the most-missed connection in the whole odyssey. In the forums, it's the single thing that most often finally produced the diagnosis.
- Community patternMine your family history. Ask relatives about psoriasis, IBD, or ‘back trouble.’ A positive family history is one of the strongest pointers patients can bring to an appointment themselves.
- Community patternGet a second opinion — don't doctor-shop. The forums' most-repeated advice, carefully framed: if a clinician dismisses a pattern that clearly fits, you are entitled to ask for a rheumatology referral or a second opinion — not to abandon care or chase a diagnosis you've decided on. The goal is the right specialist, not a doctor who'll simply agree with you.
Refuse to be dismissed. But aim for the right specialist, not just a doctor who agrees with you.
— the collective lesson
The biologic carousel
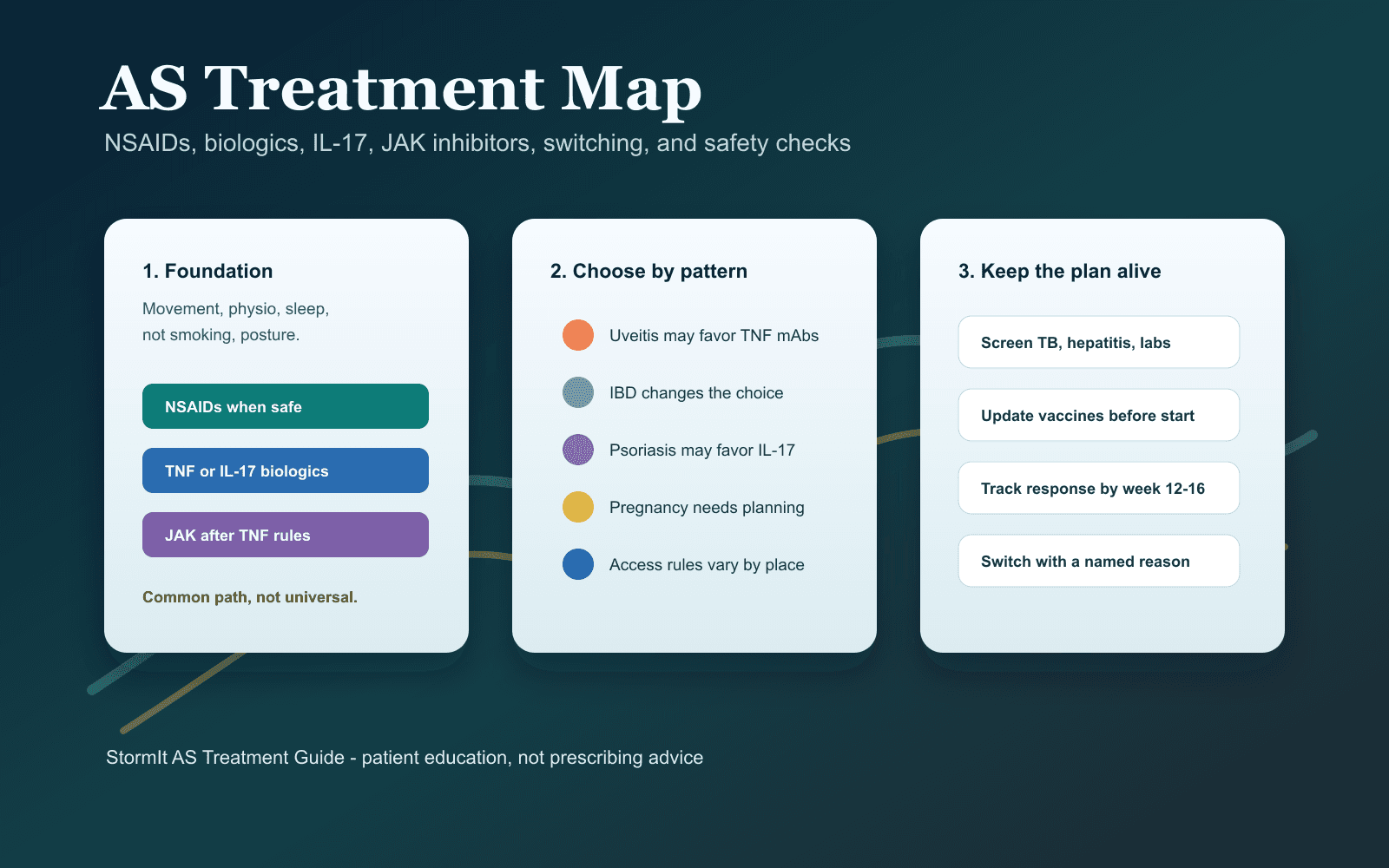
| Class | Examples | Where it fits |
|---|---|---|
| ClassTNF inhibitors | Examplesadalimumab, etanercept, infliximab, golimumab, certolizumab | Where it fitsUsual first biologic; ~40% persist at year 1[3] |
| ClassIL-17 inhibitors | Examplessecukinumab, ixekizumab | Where it fitsStrong option after TNFi failure — but flag any IBD first[4] |
| ClassJAK inhibitors | Examplestofacitinib, upadacitinib | Where it fitsOral; for persistent activity after biologics[4] |
- Moderate evidenceA fade is often immunological. When a biologic stops after a year or two, your body may have made antibodies against the drug. Ask whether trough levels and anti-drug antibody testing are appropriate before switching.
- Strong evidenceAfter two TNFi failures, switch class. Cycling endlessly within the TNF family is discouraged; guidelines support moving to a different mechanism (IL-17 or JAK) when TNF inhibitors fail[4].
- Moderate evidenceFlag gut symptoms before IL-17. Any bloody stool, persistent diarrhoea or abdominal pain matters — IL-17 inhibitors can worsen inflammatory bowel disease, so this changes the drug choice[4].
- Community patternUse the appeal templates. Insurers (US) and provincial formularies (Canada, via Special Authority) often force the cheapest drug first. Patient orgs keep appeal templates — use them[13].
- Community patternThe honeymoon crash is real. Many quietly assumed the first biologic meant ‘cured,’ then crashed when it faded. The reframe the community offers: this is chronic, and the next drug usually exists.
- AnecdotalShot anxiety fades. Patients' own tips: room-temperature the pen for 30 minutes, ice the site, inject the thigh, rotate sites. By month three most say it's routine. Comfort tips, not clinical advice.
The diet question
With that said honestly: the gut is genuinely implicated in AS. The Klebsiella–HLA-B27 molecular-mimicry hypothesis has real immunological support[5], and a 2024 review of 47 studies confirmed altered gut microbiota in AS[6]. What's missing is the trial that would tell us who responds and how much[7]. The forums skew toward responders because non-responders quietly leave — a survivorship bias worth naming out loud.
- Community patternRun it as an honest N=1. Track two weeks before changing anything. Go genuinely low-starch for 6–8 weeks, tracking daily. Then reintroduce and watch. Better-off, worse-on, repeated is your only honest evidence. If nothing changes, accept that and stop.
- Strong evidenceNever replace medication with food. Diet is an adjunct, never a substitute[7]. The patients who do best are on their biologics and eating the way their body taught them — not choosing one over the other.
- Community patternRestriction has costs — count them. Social meals and travel get harder; eating disorders can hide inside ‘anti-inflammatory’ framing. If the diet is worse than the disease, permission to stop is itself wisdom.
- Moderate evidenceMediterranean is the safe default. For those who won't go as far as no-starch, the Mediterranean pattern has the broadest evidence for inflammation and long-term health, with little downside.
- AnecdotalYour trigger may be specific — or absent. Some find it's starch; some gluten, sugar, alcohol, or ultra-processed food; many find nothing reproducible. There's no universal AS diet — only yours, found by careful experiment, if at all.
The movement discovery
- Strong evidence
- Community patternThe non-negotiable morning routine. Almost every doing-well patient describes a 10–15 minute morning routine — the daily decompression of a body that's been still for eight hours. The single most-recommended habit in the community.
- Community patternWater, more than anything. Asked what one form of exercise changed their life, the forums say swimming and warm-water hydrotherapy more than anything else. Buoyancy, warmth, full-spine movement.
- Moderate evidenceNot all movement is equal. AS is not a ‘core weakness’ problem; treating it like one — heavy sit-ups, crunches, deep forward folds, racing-posture cycling, heavy axial loading — can aggravate inflamed entheses. An AS-literate physiotherapist tailors it.
- Community patternPosture is the long game. ‘Your body fuses in the position you let it rest in’ — passed around the forums like a family heirloom. The chair, the pillow, the screen height, the sleep position: all of it compounds over decades.
The flare playbook
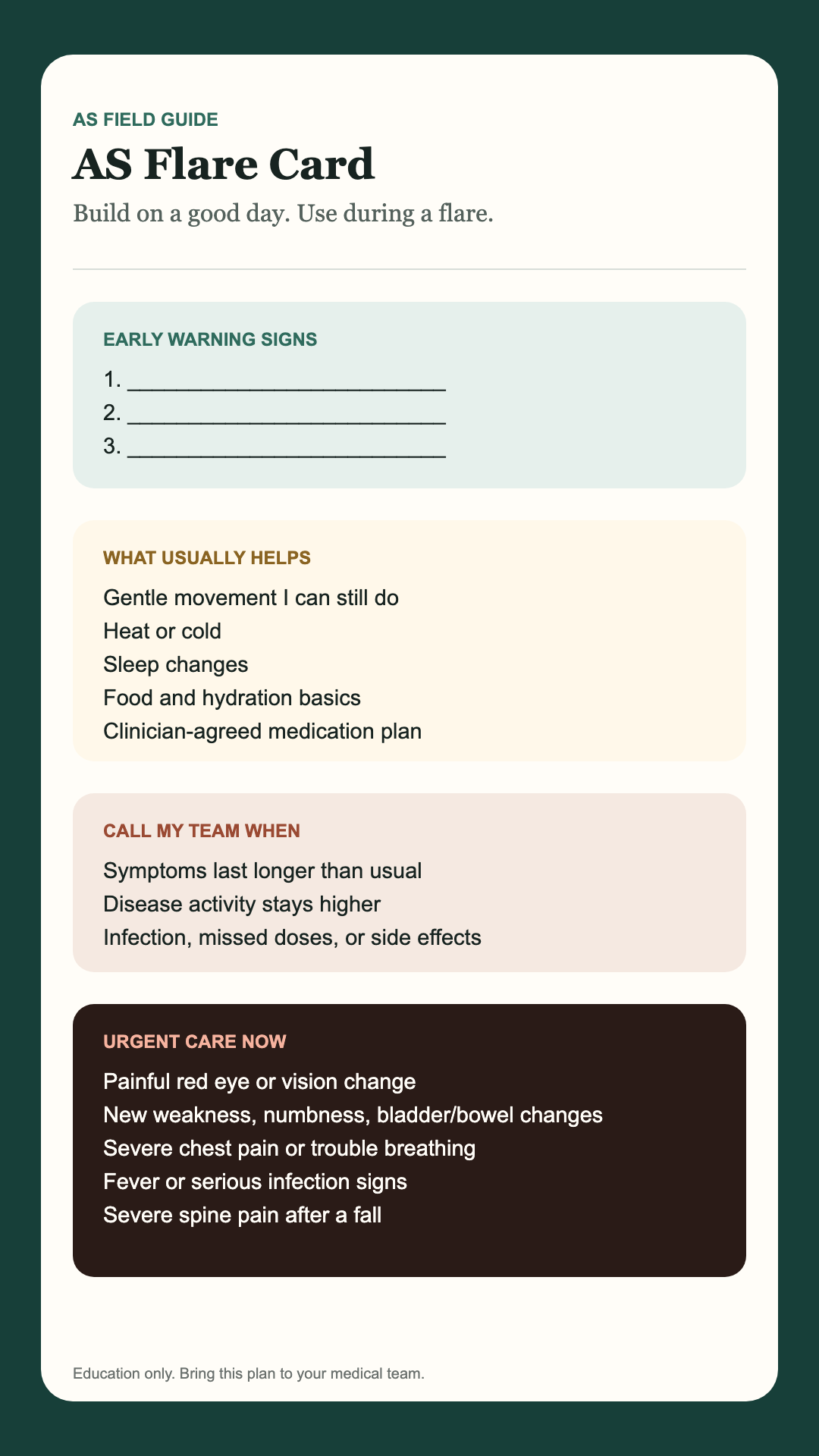
A flare is when the disease turns the volume up: pain rises, stiffness thickens, sleep breaks, energy drops, mood darkens. The community's hardest-won skill isn't avoiding flares — it's having a plan made before one, when you're calm, instead of improvising in the middle of the worst week of your month.
- Community patternRun a flare audit first. Before reacting, ask what lit it: bad sleep, a stress spike, too much sitting, overtraining, under-moving, a trigger food, a missed dose, an infection. Most flares have a fingerprint, and naming it is half the plan.
- Community patternReduce fuel, don't freeze. Scale movement down, not to zero — gentle mobility keeps a flaring spine from seizing. Heat if it helps, protect sleep, eat predictably, shed non-essential commitments, and follow the medication plan you agreed with your clinician.
- Community patternWrite the flare card before you need it. A single card made on a good day: my early warning signs, what usually helps, what worsens it, what movement I can still do, what to reduce, and when I call the doctor. A calm plan beats a heroic one made in pain.
- Moderate evidenceDon't treat every flare as a drug failure. Short flares around stress, illness or overdoing it are normal and self-limited. A sustained rise in disease activity over weeks is the signal to talk to your rheumatologist about whether treatment needs to change[4].
Sleep, the other half of the disease
Inflammatory back pain has a cruel signature: it's worst in the second half of the night and at rest. Sleep disturbance in AS is not a side issue — the scoping review of 70 studies found sleep disorders in anywhere from 2% to 72% of patients depending on the cohort and the tool[9]. Poor sleep feeds pain, pain feeds poor sleep, and the community spends a lot of words on breaking that loop.
- Community patternThe 4 a.m. wake is the disease, not you. Waking in the small hours stiff and aching is a recognised feature of inflammatory back pain, not insomnia or anxiety alone. Naming it correctly changes how you treat it.
- AnecdotalTune the sleep surface and position. The most-repeated forum fixes: a medium-firm mattress, a pillow that keeps the neck neutral, and avoiding heavily flexed (curled-up) sleep positions that the spine then sets into. Experiment; there's no single right answer.
- Community patternMove before bed and before rising. A few minutes of gentle mobility before sleep, and again before getting out of bed, blunts the worst of the morning seize-up that wrecks the last hours of sleep.
- Moderate evidenceTreat sleep as part of disease control. Persistent night pain that keeps waking you is a marker of inadequately controlled inflammation — worth raising with your rheumatologist, not just a sleep-hygiene problem[9].
The mental-health reckoning
The numbers are striking, even allowing for how widely they range across studies. A scoping review of 70 studies found depression prevalence in AS spanning 3–66%, anxiety 3–78%, and sleep disorders 2–72%[9]; meta-analysis confirms depression and anxiety are substantially more common in AS than in the general population[10]. This is one of the best-evidenced ‘hidden’ parts of the disease.
| Burden | Reported range in AS | Versus general population |
|---|---|---|
| BurdenDepression | Reported range in AS3–66% across studies[9] | Versus general populationSubstantially higher[10] |
| BurdenAnxiety | Reported range in AS3–78% across studies[9] | Versus general populationSubstantially higher[10] |
| BurdenSleep disturbance | Reported range in AS2–72% across studies[9] | Versus general populationMarkedly higher[9] |
- Moderate evidenceIt's biology, not character. Chronic systemic inflammation directly affects mood, chronic pain depletes resilience, and chronic fatigue erodes hope. The depression is real biology[10] — patients who grasp this stop blaming themselves.
- Community patternThe first three years are hardest. The grief of diagnosis, the lost imagined futures, the identity shift — most acute in the first one to three years. Those who get support through it describe the next decade as easier.
- Community patternIsolation is the multiplier. In almost every thread: silence makes everything worse. A spouse, a friend, a therapist, a forum, a stranger in a Discord — telling someone is itself part of the treatment.
- Community patternGet chronic-illness-literate therapy. Generic CBT often underwhelms; therapists trained in chronic illness, health psychology, or somatic approaches come up again and again as transformative. Ask about that experience specifically.
- AnecdotalMedication is not weakness. A recurring pattern: patients who took years to ‘give in’ to an SSRI, then wished they'd started earlier. A decision to make with your doctor — but the shame keeps people suffering longer than they need to.
Relationships, intimacy & the people around you
- Community pattern‘But you don't look sick’ erodes belief. Invisible illness slowly trains the people around you to stop believing it. Educating the people you love — once, clearly, with the fingerprint and the fatigue — is part of the long work.
- Community patternName the fatigue out loud. Pain is legible; fatigue is invisible and reads as flakiness. ‘I'm not avoiding you — my body is empty today’ lands better than a cancelled plan with no explanation.
- Community patternMind the caregiver. Spouses and parents get their own burnout and depression. The strongest partnerships are the ones where the caregiver also has friends, hobbies, and their own support.
- AnecdotalIntimacy takes planning, and that's okay. Pain, fatigue, medication effects on libido and body image all show up in the bedroom. What the forums share: timing around the morning routine, positions that don't load the spine, honest conversation, and pelvic-floor physio when it's relevant.
- Community patternParenting with AS is possible. Saving energy for the kids, explaining it age-appropriately, surviving the guilt of bad days. Most patient-parents say their children grew up more emotionally fluent, not less.
Work, disclosure & disability
- Community patternDisclosure is a calculus, not a moral. Some workplaces are safe to disclose to; some aren't. Read the room. Some patients never tell and structure life around it; some tell on day one. Both can be right.
- Moderate evidence
- Community patternMost accommodations are small. What people actually need is modest — a flexible start time, a sit-stand desk, stretch breaks, WFH on flare days, an ergonomic chair, close parking. Rarely expensive or disruptive.
- Community patternSort disability cover early. Short- and long-term disability and government programs (US SSDI; UK ESA/PIP; Canada CPP-D and provincial supports) are easier to arrange before you need them. Apply early, document everything, get an advocate if you can[16].
- AnecdotalThe pivot can be a gift. Patients who mourned a lost physical career often describe the one they pivoted into — knowledge work, advocacy, writing, teaching — as more meaningful, not less.
The long game
AS is a marathon measured in decades, and the disease you manage at 30 is not the one you manage at 55. The long-timers in the community — people fifteen, twenty, thirty years in — carry a kind of wisdom the newly diagnosed can't yet have, and they give it away freely.
- Community patternTurnarounds are combinations. Almost no one's breakthrough is a single magic bullet. It's the right biologic and a daily routine and a diet that helped and a good rheumatologist and a therapist and sleep finally fixed — several things falling into place at once. The visible piece is usually the smallest part.
- Community patternAcceptance frees energy. Many breakthroughs follow a moment — sometimes years in — when the patient stops fighting the diagnosis and starts building life around it. The fight had been eating the energy that acceptance gives back.
- Community patternThe body keeps adapting. Patients decades in describe the body finding new ways to do old things — slower, but real. Hope in a different vocabulary than ‘cure.’
- Strong evidenceYou were diagnosed in the best era yet. The treatment options of 2026 did not exist in 2010, which did not exist in 1995. Modern biologics and earlier diagnosis have genuinely changed the long-term trajectory[4] — the disease your uncle had is not the one you have.
The body is the loud problem; the community is the quiet medicine. The people who do best, over decades, use everything available to them.
— the distilled lesson
Where the communities live
If this makes you want to spend time where the wisdom actually lives, these are the places. Treat them as a complement to a good rheumatologist, an AS-literate physio, and a mental-health professional — never a replacement.
- Reddit · r/ankylosingspondylitisThe most active, candid and diverse AS community online
- Spondylitis Association of America forumsLong-running, well-moderated, often longer-form · spondylitis.org
- KickASHistorical center of the no-starch / lifestyle community · two decades of archives · kickas.org
- HealthUnlocked (NRAS & related)UK-centered, strong patient-to-patient advice
- CreakyJoints / Global Healthy Living FoundationAdvocacy + community with strong research links · creakyjoints.org
- NASS (UK)Patient organization with active community resources · nass.co.uk
- Spondylitis Association of AmericaSupport groups, disclosure & step-therapy templates · spondylitis.org
- Canadian Spondyloarthritis AssociationPatient resources & support tailored to Canada · spondylitis.ca
- Arthritis Society CanadaWorkplace, disability and medication-access guidance · arthritis.ca
- Provincial Special Authority / private insuranceHow most Canadians actually access biologics — ask your rheumatology clinic
- ‘Ankylosing Spondylitis Support’ and similarLarge, general, active — vet moderation before settling in
- ‘The Low/No Starch Lifestyle for AS’The diet-experiment community (mind the survivorship bias)
- Ankylosing Spondylitis News / BioNewsPatient-columnist platform with first-person essays on every topic here
The medicine no trial measures
Almost everything in this guide was discovered — and is still being rediscovered — by patients before it filtered into the literature. Some of it will be in the textbooks in five years. Most won't. That isn't a criticism of medicine; it's a recognition that the disease has a texture no one but another patient can fully describe.
So here is the one concrete ask of this whole piece. Find your people — pick one community from the list above this week and read other patients' stories until you recognise your own. Then, when you have a story worth telling, tell it. You will be the 2 a.m. voice for someone who is exactly where you were.
That is the medicine that doesn't appear in any clinical trial. And it is, for many people, the medicine that matters most.
References
- CreakyJoints. Ankylosing Spondylitis vs. Fibromyalgia: Could You Be Misdiagnosed?. CreakyJoints (2019). Accessed: Jul. 9, 2026. [Online]. Available: https://creakyjoints.org/about-arthritis/diagnosis/ankylosing-spondylitis-vs-fibromyalgia/
- Zhao SS, Pittam B, Harrison NL, Ahmed AE, Goodson NJ, Hughes DM. Diagnostic delay in axial spondyloarthritis: a systematic review and meta-analysis.. Rheumatology (Oxford), 60(4) (2021). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/33428758/
- Hunter T, Schroeder K, Sandoval D, Deodhar A. Persistence, Discontinuation, and Switching Patterns of Newly Initiated TNF Inhibitor Therapy in Ankylosing Spondylitis Patients in the United States.. Rheumatology and Therapy, 6(2), 207-215 (2019). Accessed: Jul. 9, 2026. [Online]. Available: https://doi.org/10.1007/s40744-019-0148-4
- Ramiro S, Nikiphorou E, Sepriano A, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update.. Annals of the Rheumatic Diseases, 82 (2023). Accessed: Jul. 9, 2026. [Online]. Available: https://doi.org/10.1136/ard-2022-223296
- Rashid T, Wilson C, Ebringer A. The link between ankylosing spondylitis, Crohn's disease, Klebsiella, and starch consumption.. Clinical and Developmental Immunology (2013). Accessed: Jul. 9, 2026. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC3678459/
- Su QY, Zhang Y, Qiao D, et al. Gut microbiota dysbiosis in ankylosing spondylitis: a systematic review and meta-analysis.. Frontiers in Cellular and Infection Microbiology, 14 (2024). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/39421642/
- Macfarlane TV, Abbood HM, Pathan E, Gordon K, Hinz J, Macfarlane GJ. Relationship between diet and ankylosing spondylitis: A systematic review.. European Journal of Rheumatology, 5(1), 45-52 (2018). Accessed: Jul. 9, 2026. [Online]. Available: https://doi.org/10.5152/eurjrheum.2017.16103
- Dagfinrud H, Kvien TK, Hagen KB. Physiotherapy interventions for ankylosing spondylitis.. Cochrane Database of Systematic Reviews, CD002822 (2008). Accessed: Jul. 9, 2026. [Online]. Available: https://doi.org/10.1002/14651858.CD002822.pub3
- Wysocki T, Mielcarska S, Kwiatkowska B, et al. Depression, anxiety, and sleep disorders in patients with ankylosing spondylitis: a scoping review.. Journal of Clinical Medicine (2023). Accessed: Jul. 9, 2026. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC10479782/
- Park JYE, Howren AM, Zusman EZ, Esdaile JM, De Vera MA. The incidence of depression and anxiety in patients with ankylosing spondylitis: a systematic review and meta-analysis.. BMC Rheumatology, 4, Article 12 (2020). Accessed: Jul. 9, 2026. [Online]. Available: https://doi.org/10.1186/s41927-019-0111-6
- Sieper J, van der Heijde D, Landewe R, et al. New criteria for inflammatory back pain in patients with chronic back pain: a real patient exercise by experts from ASAS.. Annals of the Rheumatic Diseases, 68(6) (2009). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/19147614/
- NICE. Spondyloarthritis in over 16s: diagnosis and management (NG65).. National Institute for Health and Care Excellence (2017; last reviewed 2025). Accessed: Jul. 9, 2026. [Online]. Available: https://www.nice.org.uk/guidance/ng65
- Spondylitis Association of America. Exercise, disclosure, and step-therapy appeal resources.. spondylitis.org (accessed 2026). Accessed: Jul. 9, 2026. [Online]. Available: https://spondylitis.org/
- National Axial Spondyloarthritis Society (NASS). Exercise and community resources.. nass.co.uk (accessed 2026). Accessed: Jul. 9, 2026. [Online]. Available: https://nass.co.uk/
- Canadian Spondyloarthritis Association. Patient resources and support.. spondylitis.ca (accessed 2026). Accessed: Jul. 9, 2026. [Online]. Available: https://spondylitis.ca/
- Arthritis Society Canada. Workplace, disability, and medication-access resources.. arthritis.ca (accessed 2026). Accessed: Jul. 9, 2026. [Online]. Available: https://arthritis.ca/


{kind=link}
{kind=link}