Not a real devil. Not the kind from religion or stories. I mean the kind only someone with chronic pain understands: invisible, patient, quiet when it wants to be, violent when it wakes up.
I call it the devil because that is how it felt to me. You may need a different image — a storm, a tide, a faulty alarm. The point is not fear. The point is pattern recognition.
For a long time, I did not know its name.
I only knew the pattern.
If I sat too long, it could wake up. If I ignored stiffness, slept badly, worked under too much stress, pushed my body too hard, or rested in the wrong way, it could wake up. (For me, food sometimes seemed part of the pattern too — though, as you'll see, that does not mean diet causes AS or cures it.)
And once it woke up, it was very hard to put it back to sleep.
Eventually, I learned its name.
Ankylosing spondylitis.
Even the name felt too clinical for something that had taken up so much space in my life. This was never just “back pain” for me. It was my neck locking so badly I could not turn properly. It was losing strength in my legs until walking became difficult. It was the humiliation of simple things becoming impossible. One of the worst memories I have is my wife tying my shoelaces because if I tried to bend forward, the pain would punish me.
That moment stayed with me. Not because of the shoelaces. Because of what it showed me.
I saw what ankylosing spondylitis could take from me if I did not take it seriously. It was not an idea anymore. It was sitting in front of me, challenging me, showing me a version of life where I could lose freedom one small movement at a time.
That was when I understood the deal. If I wanted to live, really live, I had to become smarter than this disease. More strategic than it.
I had to learn how to keep the devil asleep.
- AS pain often behaves backwards: rest can worsen it, movement can ease it.
- A normal X-ray, normal bloodwork, or a negative HLA-B27 does not always end the story.
- The right specialist matters — ask about inflammatory back pain and axial spondyloarthritis by name.
- Your system has four pillars: medicine, movement, food awareness, and mind — over a foundation of self-advocacy.
- Flares need a plan made before the flare.
- Red flags are not flare strategy — they are urgent-care territory (see the box below).
The Pain That Behaves Backwards
The first thing I wish I had understood is that AS pain often behaves backwards.
Most people think back pain means the body wants rest. You lie down, take it easy, wait, and hope the pain fades. But inflammatory back pain can do the opposite.
It can be worse after rest. Worse after sleep. Worse after sitting. Then, strangely, it can improve when you move.
Experts describe inflammatory back pain with features such as gradual onset, younger age at onset, improvement with exercise, no improvement with rest, and night pain that improves after getting up[1]. Primary-care guidance on axial spondyloarthritis also highlights morning stiffness, alternating buttock pain, improvement with exercise rather than rest, and good response to anti-inflammatory medication[2].
- Do I wake up stiff, and does the stiffness last more than 30 minutes?
- Is it worse after sitting or sleeping, and better when I move?
- Does pain wake me in the second half of the night?
- Did this begin before age 45, and has it lasted more than three months?
- Do I feel deep pain in my lower back, hips, or buttocks — sometimes alternating sides?
- Do anti-inflammatories (NSAIDs) help noticeably within 24–48 hours?
- Have I had heel pain, rib pain, a swollen finger or toe, psoriasis, gut inflammation, or an episode of eye inflammation?
- Does anyone in my family have AS, psoriasis, IBD, or related inflammatory disease?
Those last items matter: NICE referral criteria for axial spondyloarthritis weigh exactly these clues — back pain starting before 45 and lasting over three months, night waking, buttock pain, improvement with movement, NSAID response, family history, enthesitis, arthritis, and psoriasis[4].
If the answer is yes to several of these, do not just “wait and see.” Write it down. Bring it to a doctor. Ask whether this could be inflammatory back pain or axial spondyloarthritis.
The goal is not to diagnose yourself. The goal is to stop dismissing the pattern.
Why Waiting Is Dangerous
The most dangerous thing I did was wait. Not because I was lazy. Because I did not know what I was waiting on. I thought stiffness would pass like a pulled muscle. I thought pain was something to endure. I thought I was being strong.
But AS is not impressed by silent suffering.
Diagnostic delay is a major problem in axial spondyloarthritis. A systematic review and meta-analysis found a pooled mean diagnostic delay of 6.7 years between symptom onset and diagnosis[3]. That is not a small delay. That is years of pain, confusion, missed treatment, and sometimes preventable damage.
Part of the problem is that early AS can hide. X-rays may be normal early. Blood inflammation markers such as CRP or ESR may be normal. HLA-B27 can support the diagnosis, but it is not a yes-or-no answer. Some people with AS are HLA-B27 negative, and many who are HLA-B27 positive never develop AS. NICE specifically says axial spondyloarthritis can be present even when X-rays show no sacroiliitis and even when HLA-B27 is negative — and that you should not rule it out on a negative HLA-B27 or normal CRP/ESR alone[4].
A normal X-ray does not always close the case. A negative HLA-B27 does not always close the case. Normal CRP and ESR do not always close the case. The story, the pattern, the exam, imaging, labs, and rheumatology judgement all matter.
— the line I most wish I'd had
So if your symptoms fit the pattern, one normal test should not end the conversation.
What AS Actually Is
Ankylosing spondylitis is a chronic inflammatory disease that mainly affects the spine and sacroiliac joints, where the lower spine meets the pelvis. It can also affect other joints, tendon and ligament attachment points, the ribs, hips, eyes, skin, and gut[5].
The disease is part of a wider family called axial spondyloarthritis, often shortened to axSpA. Some people have visible structural changes on X-ray, historically called ankylosing spondylitis or radiographic axSpA. Others have symptoms and inflammation that may be visible on MRI but not yet on X-ray, called non-radiographic axial spondyloarthritis[4][6].
AS is not just back pain. It is immune-driven inflammation.
And when inflammation keeps burning around the spine and pelvis, it can cause pain, stiffness, reduced mobility, and in some cases structural damage or fusion over time. Not everyone develops severe fusion, and modern treatment can help many people control disease activity, but waiting and guessing is not strategy[6][7].
The Doctor Conversation That Changes Everything
Do not walk into the appointment trying to sound like a medical textbook. Walk in with the pattern.
- “I have had lower back, hip, or buttock stiffness for more than three months. It is worse in the morning and after rest. It improves when I move. Sometimes it wakes me at night. I am worried this may be inflammatory back pain or axial spondyloarthritis.”
- “I think I have ankylosing spondylitis.”
That sentence is powerful because it gives your doctor clinical clues, not just fear.
- “Do my symptoms sound like inflammatory back pain?”
- “Should I be referred to a rheumatologist?”
- “If my X-ray is normal, would an MRI of the sacroiliac joints be appropriate?”
- “Should we test HLA-B27, CRP, and ESR?”
- “What should I track before my next appointment?”
A prepared patient is not a difficult patient. A prepared patient helps the doctor see the signal through the fog.
The Four Pillars
Living with AS is not one action. It is a system. For me, the system became four pillars over a foundation of self-advocacy.
Not all four pillars do the same job. They are not interchangeable. You cannot replace medical treatment with diet. You cannot replace movement with medication. You cannot replace sleep and stress management with willpower. But together, they create a life where the disease has fewer places to hide.
The clinical foundation
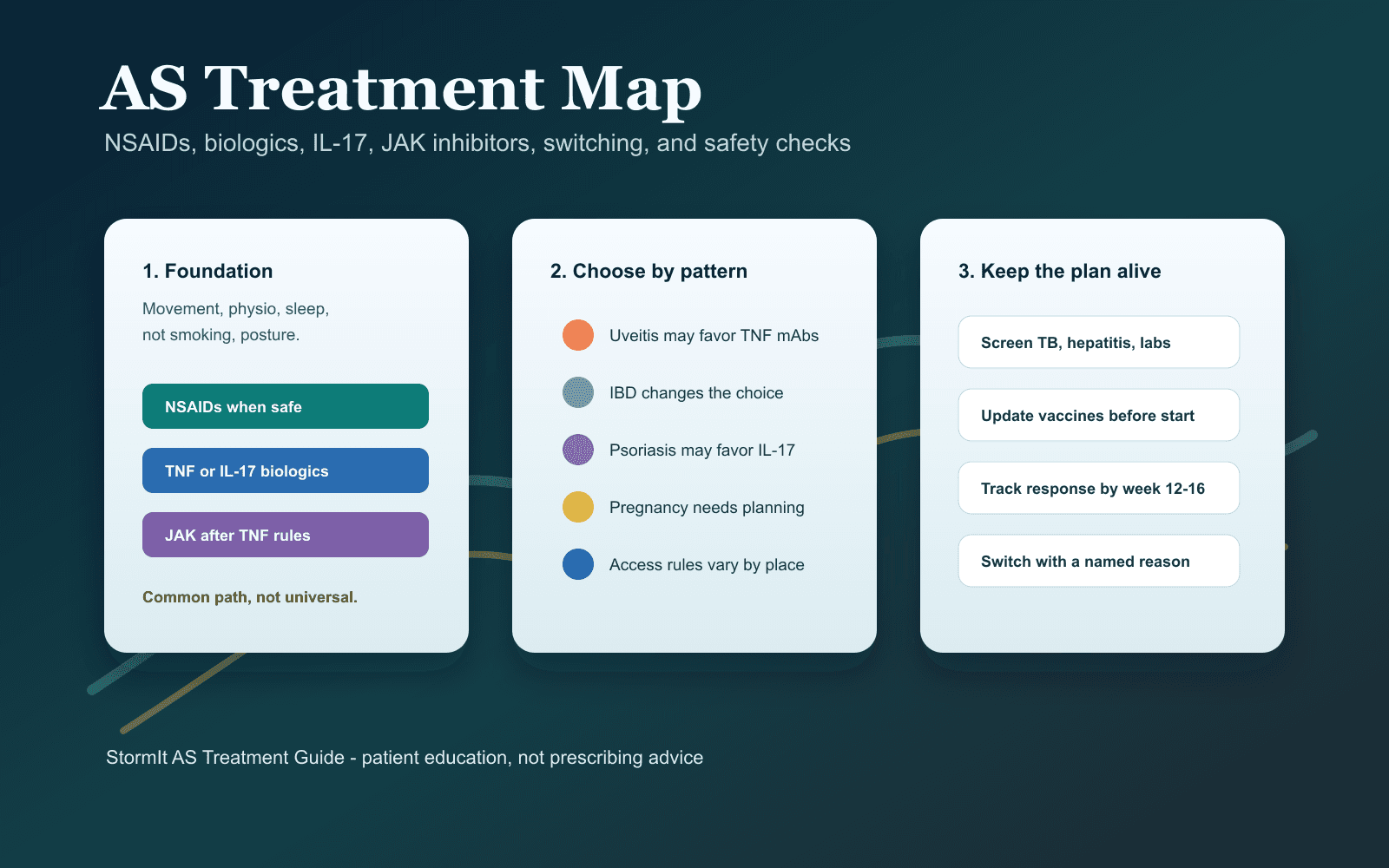
Major recommendations for axial spondyloarthritis include education, exercise, NSAIDs when appropriate, monitoring, and advanced therapies such as TNF inhibitors, IL-17 inhibitors, and, in selected cases, JAK inhibitors when disease activity remains high[7][9].
This does not mean everyone needs the same medication. It means AS should be managed with a rheumatologist and monitored properly. For many people, medication is what makes movement possible — it quiets the biological fire enough for the rest of the system to work.
If your disease is aggressive, needing medication does not mean you failed. It means the disease is real.
How you protect function
For most people with AS, the question is not whether movement matters — every major guideline recommends exercise and physiotherapy, and Cochrane evidence suggests home-based or supervised programs beat no intervention[10][12]. The question is what kind, how much, and when — movement has to match the body in front of you. This is intelligent movement, not punishing the body.
- Gentle spinal mobility & hip mobility
- Chest expansion and breathing
- Posture work
- Walking or low-impact cardio
- Strength training adapted to your body
- Flare-day movement that is smaller but not zero
On good days, you build capacity. On bad days, you keep the bridge open. A flare is not the day to prove your toughness.
Experiment, don't panic
Some AS communities talk about low-starch diets, often connected to theories about gut bacteria. The gut connection is a serious area of research[13], but the evidence for specific diets remains limited and inconclusive[14].
So the honest position: food may matter for you. Food is not proven to cause or cure AS. A diet experiment should never replace medical care. Test it like a scientist — track a baseline, change one thing at a time, give it a defined window, judge the data honestly.
If a diet becomes so restrictive that it damages nutrition, mood, or social life, that is not healing. Permission to stop is itself wisdom.
The command center
AS is not “in your head.” The inflammation is real. But the mind is still involved — not as the cause, as the command center. It decides whether you track or ignore, move or freeze, sleep or scroll, stop before stress becomes a storm.
People with AS have increased risk of depression and anxiety, and mental health should be treated as part of care, not as a character flaw[15].
For me, this meant learning to notice early warning signs before they became punishment: a shift in fatigue, restless sleep, a strange stiffness, a mood change, the quiet sense that something was beginning to turn. The goal is vigilance without fear.
Respect the disease without worshipping it. Pay attention without making AS the center of your identity. Build routines, but still live. Keep the devil asleep, but do not spend your whole life staring at its bedroom door.
The Flare Plan
A flare is when the disease turns the volume up. Pain rises. Stiffness thickens. Sleep breaks. Energy drops. The mind gets darker. The body becomes expensive to operate.
Your job during a flare is not to panic. Your job is to reduce fuel.
- Did I sleep badly?
- Did stress spike?
- Did I sit too long?
- Did I overtrain?
- Did I stop moving?
- Did I eat something that often causes trouble?
- Did I ignore early stiffness?
- Did I miss medication or change routine?
- Move gently, but do not go completely still.
- Use heat if it helps. Scale down exercise intensity.
- Protect sleep. Eat predictably. Reduce commitments where possible.
- Follow your medication plan from your clinician.
- Contact your doctor if the flare is severe, unusual, prolonged, or different from your normal pattern.
Red Flags: When Not to Wait
Most AS symptoms are part of the long game. Some are not. (This repeats the box near the top — on purpose. It is the one part of this guide that can't wait.)
- A painful red eye, light sensitivity, or vision changes — uveitis can require same-day assessment[16].
- New leg weakness, numbness, or loss of bladder or bowel control.
- Severe chest pain or trouble breathing.
- Fever or signs of serious infection, especially if you are on immune-modifying medication.
- Sudden severe back or neck pain after a fall, jolt, or trauma — especially in advanced or fused disease.
The AS Starter Kit
If this guide gives you only one thing, let it be this: stop living randomly. Build a kit. Here is the whole thing on one screen — screenshot it, then read the detail below.
- Pain 0–10 · morning stiffness (min)
- Sleep · fatigue · stress 0–10
- Movement · food notes · medication
- Eye / skin / heel / rib / joint / gut
- When & where it started; better/worse
- Morning stiffness length; night waking
- Family history; the symptoms above
- Medication response + your top 3 questions
- My early warning signs are…
- What helps · what worsens it
- Movement I can still do · what to reduce
- When I call the doctor · what means urgent care
- 5–10 min walking
- Gentle spinal & hip mobility
- Breathing into the ribs
- A warm shower; break up long sitting
Track a baseline first. Change one variable. Give it a defined window. Judge honestly — the goal is to learn your own body without harming it, not to win an argument about starch.
The detail, if you want to build each one out:
- Pain 0–10
- Morning stiffness (min)
- Sleep quality
- Fatigue
- Movement
- Stress 0–10
- Food notes
- Medication
- Gut symptoms
- Eye / skin / heel / rib / joint
- When symptoms started — and where pain occurs
- What makes it worse, what makes it better
- How long morning stiffness lasts; whether it wakes you
- Family history; eye, gut, skin, heel, rib, joint symptoms
- Medication response
- Your top three questions
- Five to ten minutes of walking
- Gentle spinal mobility & hip mobility
- Breathing into the ribs
- A warm shower
- Short movement breaks during long sitting
- My early warning signs are:
- What usually helps:
- What usually worsens it:
- What movement I can still do:
- What I should reduce:
- When I call the doctor:
- What symptoms mean urgent care:
Go Deeper — The Rest of the AS Series
This piece is the front door. When you're ready to go further, each pillar has its own full guide:
Medicine · the treatment mapTreating Ankylosing Spondylitis in 2026→
Movement · the physiotherapy manualMove or Fuse→
The human side · lived-wisdom encyclopediaThe Things You Only Learn From the AS Community→
Food · eating for inflammationWhat We Eat→
Solution-Focused Resources
Use resources that help you act, not just worry.
- DiagnosisNICE NG65 & NIAMS. NICE gives practical guidance on recognizing and managing spondyloarthritis in people over 16; NIAMS explains diagnosis, tests, and treatment in patient-friendly language.[4][5]
- Primary careThe Mayo Clinic Proceedings guide on recognizing axial spondyloarthritis explains the inflammatory back pain pattern in terms clinicians understand.[2]
- TreatmentThe ASAS-EULAR, ACR/SAA/SPARTAN, and 2025 British Society for Rheumatology recommendations show how specialists think about NSAIDs, biologics, targeted therapies, monitoring, and escalation.[7][9]
- MovementThe National Axial Spondyloarthritis Society and Spondylitis Association of America provide practical exercise resources designed for axSpA and AS.[11][12]
- Disease activityThe Spondylitis Association of America's BASDAI calculator helps you understand one common disease-activity tool used in AS.[17]
- CanadaThe Canadian Spondyloarthritis Association offers patient resources, guidebooks, and support for people living with spondyloarthritis.[18]
- DietBegin with evidence reviews, not influencers. Macfarlane et al. concluded that evidence on diet and AS is extremely limited and inconclusive — exactly why diet should be a careful personal experiment, not a universal cure.[14]
- EyesKnow the emergency rule: a painful red eye, light sensitivity, or vision change should be assessed urgently. NHS uveitis guidance and the SAA's uveitis resource are useful starting points.[16]
- Mental healthChronic pain can make the room feel very small. If you are in immediate danger, call emergency services. In Canada, call or text 9-8-8; in the U.S., call, text, or chat 988 for 24/7 crisis support.[19][20]
What I Wish I Knew Earlier
- I wish I knew that rest making pain worse was a clue.
- I wish I knew that morning stiffness was not just age, posture, or a bad mattress.
- I wish I knew that a normal X-ray did not always close the case.
- I wish I knew that HLA-B27 was important, but not destiny.
- I wish I knew that medication was not weakness.
- I wish I knew that movement mattered, but had to match my body that day.
- I wish I knew that food might matter, but food fear can become its own prison.
- I wish I knew that mental training was not motivational fluff — it was part of the daily architecture.
AS did not only teach me pain. It taught me strategy. It taught me that ambition without recovery is just self-destruction in a better suit. It taught me that the body whispers before it roars. It taught me that every small success matters.
The body whispers before it roars.
— the one line I'd put on a wall
Every walk.
Every stretch.
Every honest appointment.
Every careful meal.
Every night of sleep protected.
Every stress storm calmed before it becomes fire.
Every moment I choose care over denial.
The devil may not disappear. But it can be weakened. Through medicine, through movement, through food awareness, through mental training — through learning your body so well that you hear the whisper before the roar.
Not perfection. Not panic. Not pretending.
A life where the devil remains asleep.
References
- J. Sieper et al., “New criteria for inflammatory back pain in patients with chronic back pain,” Annals of the Rheumatic Diseases, vol. 68, no. 6, pp. 784–788, 2009, doi:10.1136/ard.2008.101501.
- M. N. Magrey, A. S. Danve, J. Ermann, J. A. Walsh, “Recognizing axial spondyloarthritis: A guide for primary care,” Mayo Clinic Proceedings, vol. 95, no. 11, pp. 2499–2508, 2020, doi:10.1016/j.mayocp.2020.02.007.
- S. S. Zhao et al., “Diagnostic delay in axial spondyloarthritis: A systematic review and meta-analysis,” Rheumatology, vol. 60, no. 4, pp. 1620–1628, 2021.
- National Institute for Health and Care Excellence, “Spondyloarthritis in over 16s: diagnosis and management,” NICE Guideline NG65, 2017.
- National Institute of Arthritis and Musculoskeletal and Skin Diseases, “Ankylosing Spondylitis: Diagnosis, Treatment, and Steps to Take,” 2023.
- K. J. Wenker, M. Q. Quint, “Ankylosing Spondylitis,” StatPearls, National Library of Medicine, updated 2023.
- S. Ramiro et al., “ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update,” Annals of the Rheumatic Diseases, vol. 82, no. 1, pp. 19–34, 2023, doi:10.1136/ard-2022-223296.
- M. M. Ward et al., “2019 Update of the ACR/SAA/SPARTAN recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis,” Arthritis Care & Research, vol. 71, no. 10, pp. 1285–1299, 2019, doi:10.1002/acr.24025.
- S. S. Zhao et al., “The 2025 British Society for Rheumatology guideline for the treatment of axial spondyloarthritis,” Rheumatology, 2025, doi:10.1093/rheumatology/keaf089.
- H. Dagfinrud, T. K. Kvien, K. B. Hagen, “Physiotherapy interventions for ankylosing spondylitis,” Cochrane Database of Systematic Reviews, 2008.
- National Axial Spondyloarthritis Society, “Exercise.”
- Spondylitis Association of America, “Spondyloarthritis and Exercise.”
- Z. Y. Song et al., “Role of the microbiome and its metabolites in ankylosing spondylitis,” Frontiers in Immunology, 2022.
- T. V. Macfarlane et al., “Relationship between diet and ankylosing spondylitis: A systematic review,” European Journal of Rheumatology, 2018.
- J. Y. E. Park et al., “The incidence of depression and anxiety in patients with ankylosing spondylitis: A systematic review and meta-analysis,” BMC Rheumatology, vol. 4, art. 12, 2020.
- National Health Service, “Uveitis”; National Institute for Health and Care Excellence, acute anterior uveitis same-day ophthalmology assessment; Spondylitis Association of America, “Iritis or Anterior Uveitis.”
- Spondylitis Association of America, “BASDAI Score Calculator.”
- Canadian Spondyloarthritis Association, “Resources for Living Better.”
- 9-8-8: Suicide Crisis Helpline Canada, “Call or Text 9-8-8,” 2026. Available: https://988.ca/
- 988 Suicide & Crisis Lifeline, “If you need emotional support, reach out to the national mental health hotline: 988,” 2026. Available: https://988lifeline.org/