
A word before we begin
If you spend twelve hours a day folded over a laptop and eight hours curled tight in bed, those positions become the ones your nervous system and connective tissues know best. If you move every joint through its available range, sit tall when you can, sleep flatter when your body allows it, and walk most days, you are giving your spine and chest wall a different set of options. Medication, inflammation, genetics, access to care, and luck all matter. Movement is simply the lever you can touch every morning.
Medication helps calm inflammation. Movement helps preserve the shape and range you live in.
— if you take one sentence from this, take this one
Why movement is medicine
Most people are told “exercise is good for you.” That isn't enough. In AS, exercise is doing seven distinct, mechanistically different things — and understanding each changes how you train. Every major guideline now puts structured exercise at the foundation of AS care, alongside medication, not after it[8][7].
- 1 · controls inflammationIn a 2016 RCT, six months of structured exercise lowered serum calprotectin and improved ASDAS-CRP in both AS and nr-axSpA[1]. Contracting muscle releases anti-inflammatory signals; your training session is, molecularly, talking down the systems attacking your spine.
- 2 · protects the working shapeYour spine may or may not fuse, and treatment can change that story. The practical movement lesson is simpler: the positions you practice daily influence the range, posture, and confidence you keep. Extension helps you look ahead and breathe; endless flexion does not.
- 3 · protects the chest & lungsAS attacks the costovertebral and costosternal joints; untreated, chest expansion shrinks toward 1–2 cm. A year of structured Pilates improved chest expansion by ~88% in one cohort[9]. Breathing well is a primary reason to exercise, not a side-effect.
- 4 · protects the heartAS is associated with higher cardiovascular risk — inflammation, medication burden, and inactivity all matter[10]. Aerobic exercise helps counter several of those risks; an aerobic-exercise RCT improved VO₂max, BASDAI and BASMI in a 12-week program[6].
- 5 · treats fatigue & low moodAbout one in three AS patients has clinically significant depression, and most describe fatigue as a major burden; structured programs produce clinically meaningful quality-of-life gains[11].
- 6 · builds the muscular corsetWhen discs and ligaments are inflamed and unreliable, the deep stabilizers (multifidus, transverse abdominis, deep neck flexors) keep the spine functional. They atrophy within weeks of reduced activity; targeted work rebuilds them.
- 7 · gives you agencyAS brings a profound loss of control. Daily movement is the one thing the disease cannot take from you — and patients who do it consistently report better mental health than equivalent patients who don't.
Start here: your first four weeks
The full program later in this guide is the destination, not the on-ramp. Newly diagnosed or in a lot of pain? Going from zero to the complete weekly plan on day one buys you a flare and a quit. Build the habit first, then the volume. Here is a gentle four-week ramp — clear it with your physio and adjust to your body.
| Week | Daily | Add this week |
|---|---|---|
| WeekWeek 1 | DailyThe 10-min morning routine, every day | Add this weekNothing else. Just land the habit. |
| WeekWeek 2 | DailyMorning routine + a 15-min daily walk | Add this weekPosture resets every hour you sit (chin tucks) |
| WeekWeek 3 | DailyRoutine + 20–30-min walk | Add this weekOne gentle strength session (bridges, bird-dogs, dead bugs) |
| WeekWeek 4 | DailyRoutine + walk | Add this weekOne swim or aquatic/yoga class; add a second strength day |
The morning stiffness window
Inflammatory back pain has a signature: worse with rest, better with movement. Inflammation pools in immobile joints overnight, so you wake stiff — not because anything new is wrong, but because nothing has moved for eight hours. NSAIDs relieve it partly; movement relieves it fully. The practical implication: build your day around a non-negotiable 10–15 minute morning routine — the single most evidence-supported daily habit in AS.
- Hot shower on lower back & neck
- Or a heating pad while still in bed
- Inflammation hates heat — use it
- Cat-cow ×10 (flex / extend)
- Thoracic rotations ×10 each side
- Kneeling hip-flexor stretch
- Standing back extension ×10
- Chin tucks against the wall ×10
- Wall stand: head, shoulders, hips, heels
- Glute bridges ×10
- 5 maximal-inhale breaths (open ribs)
- Stand tall, chest up, shoulders back
- Pain is often substantially reduced
Patients who do this daily for a year report dramatically less pain, better posture, and almost never the “where did the day go, I haven't moved” crash that catches sedentary people by 4 pm.
The seven pillars
Generic advice — “walk more, stretch a bit” — won't get you where you need to be. A proper AS program touches seven distinct domains, each with its own purpose and dose. Most patients do one or two well and ignore the rest.
Pillar 1 · Spinal mobility — every segment, every direction, every day
The spine has six movements: flexion, extension, lateral flexion left and right, and rotation left and right. AS fuses joints in whichever direction you don't take them. The rule: every segment travels through its full available range every single day.
- cat-cow ×10Flexion and extension of the whole spine, on hands and knees.
- thoracic rotations ×10Sitting cross-legged, rotate the trunk each way — frees the often-stiff mid-back.
- standing back extension ×10Hands on hips, gently arch backward. The most important movement — AS preferentially loses extension.
Pillar 2 · Postural training — where the long-term battle is fought
Posture is mostly built in the hours you don't think you're exercising — at the desk, in the car, on the sofa. The goal is not perfection. It is frequent, gentle resets before stiffness becomes the default.
- wall standDaily: head, shoulders and buttocks touching the wall, heels 5–10 cm out, 30 seconds. If your head won't easily touch, that's the first thing to fight for.
- chin tucksPull the head straight back (a ‘double chin’), not down — the antidote to forward-head posture. Ten reps, several times daily.
- tragus-to-wallA standard AS metric your physio should track. Movement keeps it small; hunched sitting grows it.
Pillar 3 · Strengthening — the muscular corset
The deep, slow muscles fail first in AS. Big surface muscles aren't the priority — the posterior chain and deep stabilizers are.
- Back extensors (erector spinae, multifidus) — superman lifts, bird-dogs, supervised deadlifts
- Glutes — bridges, hip thrusts, banded monster walks
- Deep core — dead bugs, pallof presses, side planks
- Scapular stabilizers & deep neck flexors — Y-T-W raises, face pulls, chin tucks against resistance
- Sit-ups, crunches, full forward bends — they reinforce the flexed posture many AS programs are trying to balance
- Heavy axial loading without supervision
- High-impact landings — running on hard surfaces, jumping, contact sport during flares
Pillar 4 · Aerobic conditioning — cardiovascular protection
AS is associated with higher cardiovascular risk; consistent aerobic work is one practical countermeasure[10]. Aim for at least 150 minutes/week of moderate cardio (or 75 of vigorous), across 3–5 sessions, adjusted to your disease activity and medical advice.
- swimmingGold standard — water unloads the spine, backstroke and freestyle reinforce extension, the breathing trains the chest wall.
- walkingUniversally available, low-risk. Brisk pace, good posture, 30 minutes is the floor.
- HIIT (with a blessing)A multicentre axSpA trial found three months of supervised high-intensity exercise reduced disease activity[2]. Treat that as a specialist-supervised option, not a start-alone challenge; get a physio's sign-off.
Pillars 5–7 · Stretching, breathing, balance
- stretchingAS attacks entheses — Achilles, plantar fascia, hip flexors, pec insertions. Hold key stretches (hip flexors, hamstrings, pecs, calves, glutes) 30 seconds, breathing through, no bouncing.
- breathingThe most under-practiced category. Five minutes daily: maximal-inhale breaths, diaphragmatic breathing, lateral rib expansion with a band. Measure chest expansion monthly — loss is an early signal to bring to your physio or rheumatologist.
- balanceIncreasingly important the longer you have AS. Single-leg stands, tandem walks, tai chi. A fall in a fused spine is catastrophic — the spine can't absorb impact through flexion.
Best modalities
The most rigorous comparative evidence comes from network meta-analyses that rank interventions across trials. Here's what they consistently find.
- 🥇 aquatic therapyA 2025 network meta-analysis ranked aquatic stretching highest for BASDAI, BASFI and ASQoL (SUCRA 85.5 / 99.6 / 88.4%)[3]. Buoyancy unloads the spine, warm water relaxes muscle, and water gives resistance without weights. The catch is access — true hydrotherapy pools are rare; NASS and SAA keep directories[12][13].
- 🥈 Pilates (mat, posture-led)Eight to twelve weeks of structured, breath-coordinated Pilates improves BASDAI, BASMI, chest expansion and quality of life[9]. Skip the high-flexion variants (rolling like a ball, deep C-curves) — an AS-literate instructor modifies these.
- 🥉 aerobic + stretching combosCombination programs beat single-modality ones: aerobic + Pilates best for BASDAI/BASMI, aerobic + stretching best for chest expansion[4]. Don't do just one thing.
- yoga — with caveatsReal value for flexibility, balance and breath — but favor extension over flexion, avoid headstands/shoulder stands and deep folds. Iyengar and restorative styles are friendliest; tell the teacher you have AS.
- tai chi — quietly excellentTop-ranked for balance and fall prevention with negligible injury risk. If a class is accessible, it touches mobility, balance, breath and meditation at once.
A complete weekly program
Once the habit is built, here is an evidence-based week that covers all seven pillars — about 5–7 hours, plus the daily morning routine. Adapt it, don't worship it, and show it to your physiotherapist to customize.
| Day | Focus | Session (≈ time) |
|---|---|---|
| DayMon | FocusStrength | Session (≈ time)30 min — back extensions, glute bridges, dead bugs, bird-dogs, band rows |
| DayTue | FocusAerobic + breath | Session (≈ time)30–40 min brisk walk or swim; finish with 5 min maximal-inhale breathing |
| DayWed | FocusAquatic or class | Session (≈ time)45 min hydrotherapy or an AS-friendly yoga / Pilates class |
| DayThu | FocusStrength | Session (≈ time)30 min — rotate Monday's work, new angles, add resistance |
| DayFri | FocusAerobic + balance | Session (≈ time)30 min cardio + 10 min balance (single-leg stands, tai chi) |
| DaySat | FocusLong active session | Session (≈ time)60–90 min — hike, longer swim, bike, dance; something fun, social if you can |
| DaySun | FocusRecovery + flexibility | Session (≈ time)30 min gentle stretching, foam rolling, restorative yoga; sauna or hot bath |
- BASDAI drops, sleep improves, energy rises — the program is working.
- Soreness for a day after a session is normal; it fades.
- Range of motion and chest expansion hold or improve month to month.
- Pain progressively worsens over weeks (not just post-session soreness) — too hard, or the wrong exercises.
- A specific movement reliably triggers a flare — drop it, ask your physio for a swap.
- Escalating daily pain is never the goal — pull back to the last volume that felt sustainable.
Flare management
Flares are not the time to stop moving. They're the time to shift to the lowest sustainable dose of the right movements until the storm passes. The body that doesn't move during a flare emerges worse than it entered.
- don't stop entirelyEven 10 minutes of gentle mobility is medicine. The body adapts to disuse within days — a week of nothing can set you back a month.
- drop to flare-day workThe morning routine slower and gentler (in bed or the shower), pool walking, gentle stretching in a hot bath, diaphragmatic breathing, a short slow walk.
- heat, not iceAS is inflammatory at a different level than acute injury — heat helps; cold often worsens the stiffness.
- sleep over volumeDuring a flare, prioritize sleep over hitting weekly numbers. Recovery is part of the program.
- call your rheumatologistA flare that won't settle in a week or two with rest and gentle movement may mean your medical regimen needs adjusting. Don't suffer through alone.
- the 10% rule backOnce it passes, add ~10% of volume back per week — not all at once.
Red flags: when to stop and seek care
Most AS symptoms are part of the long game you manage with movement. A few are not, and exercising through them is dangerous. Learn this short list and act on it fast.
The other 22 hours
You can do everything right for two hours a day and undo it with the other twenty-two — especially the eight in bed. The position the spine sleeps in is the position it spends most of its life in.
Sleep · Default to flat
- on your back, thin pillowSleep ‘as flat as possible’ to encourage extension and prevent flexion contractures. One pillow under the knees can ease lumbar strain.
- avoid the foetal curlThat position can reinforce the flexion you are trying to balance. Side-sleepers: a pillow between the knees and a thicker neck pillow to keep alignment.
- firm mattressMemory foam that creates a ‘valley’ lets the spine sag into bad positions.
Desk, car, lifting · Engineer the day
- Monitor at eye level; keyboard at elbow height; lumbar support behind the lower back
- Sit-stand desk if possible — alternate every 30–60 minutes
- Every 25 minutes: stand, five chin tucks, a minute's walk (set a timer)
- Driving: lumbar roll, upright seat, mirrors set so a slouch hides them
- On flights: aisle seat, walk hourly, seated thoracic rotations
- Lift from hips and knees, never the lumbar spine; carry loads close
Mistakes that make AS worse
The patient who exercises with bad mechanics is sometimes worse off than the one who doesn't exercise at all. The most common mistakes:
- generic gym coreSit-ups, crunches, flexion ‘ab work’ reinforce the posture many AS patients are trying to balance. Replace with anti-flexion work — dead bugs, bird-dogs, planks, pallof presses.
- racing-posture cyclingThe forward-leaning road-bike position can feed the rounded shape you are trying not to live in all day. Switch to an upright/hybrid or recumbent bike.
- stopping during flaresModify, don't quit. Disuse undoes you fast.
- pushing through sharp painInflammatory ache is different from injury pain. New sharp pain = stop, reassess, possibly see your physio.
- only what feels goodMost people do their favorite one or two pillars and skip the rest. Touch all seven.
- no warm-upCold AS tissue tears more easily than cold healthy tissue. Always start with 3–5 minutes of light movement.
- comparing to a ‘normal’ bodyYour full range may be smaller. Your range is what you train — maintaining your own ceiling matters far more than reaching someone else's.
Finding a physio who knows AS
A great AS physio changes everything. A generic one who treats your back like a normal back can actively harm you. This is the most important practical relationship in your movement life — here's how to find and vet one.
- Specific experience with AS / axial spondyloarthritis — ask how many they currently see
- Fluency in BASMI, BASDAI, BASFI measurements
- A focus on extension and posture, not generic ‘core strengthening’
- A long-term partnership orientation and willingness to coordinate with your rheumatologist
- Heavy emphasis on passive treatments (massage, ultrasound, e-stim) without active exercise
- Generic ‘strengthen your core’ with crunches and sit-ups
- No awareness of the extension/flexion distinction
- Aggressive spinal manipulation in active AS; one-size-fits-all plans
The vetting call · Five questions to ask before you book
- “How many patients with axial spondyloarthritis do you currently treat?”
- “Do you track tragus-to-wall and chest expansion, or use BASMI?”
- “Will my program prioritize extension and posture over generic core work?”
- “Will you coordinate with my rheumatologist and adjust around flares?”
- “Do you offer tele-rehab so I can keep going when I travel or flare?”
The future & special cases
The next decade · Wearables, tele-rehab, AI
- wearable-assisted programsA 2022 RCT delivered a home program by smartwatch + app; the intervention group beat controls on ASDAS, BASDAI, BASFI, BASMI, chest expansion and VO₂max — at 84% adherence[5].
- tele-rehabilitationSince 2020, video-supervised PT has been validated as roughly equivalent to in-person care for many patients, vastly improving access — especially outside big cities.
- AI-personalized prescriptionEarly systems adjust your program from BASDAI, wearable data and symptoms — easing back at flare risk, pushing when recovery markers are good.
Life phases · When the picture changes
- pregnancyKeep moving throughout — swimming and prenatal yoga are excellent; avoid supine after the second trimester. Rebuild gradually postpartum, prioritizing pelvic floor and deep core.
- advanced fusionPrinciples unchanged, execution adapts: hydrotherapy and balance work become central; chair- and bed-based versions keep the morning routine alive. An AS-specialist physio is essential.
- active uveitisAvoid head-down positions — no inversions, downward dogs or aggressive forward folds — until the eye settles.
- older patients (60+)Bone health becomes a parallel priority — osteoporosis is common in long-standing AS. Add weight-bearing work, prioritize fall prevention, ensure vitamin D and calcium.
The mini-directory
Working starting points — organizations, evidence, and the small kit that replaces most of a gym. Treat forums as hypotheses to test with your physio; treat the trials and society resources as ground truth.
- NASS — National Axial Spondyloarthritis Society (UK)‘Back to Action’ program + hydrotherapy & physio directories · nass.co.uk
- Spondylitis Association of AmericaExercise videos, aquatic rehab, ‘Prescription for Exercise’ · spondylitis.org
- Physiopedia — AS exercise pageWritten for clinicians, dense with evidence
- Canadian Spondyloarthritis AssociationPatient resources tailored to Canada · spondylitis.ca
- Arthritis Society CanadaPhysio access, workplace & self-management guidance · arthritis.ca
- Public vs private physiotherapySome public/hospital coverage by province; private clinics via extended benefits, usually shorter waits
- Reddit · r/ankylosingspondylitisLarge peer forum for AS/axSpA lived experience; verify any exercise or medication claim.
- Facebook · Ankylosing Spondylitis Support & InformationSearch the exact group name; prefer groups with active moderation and no miracle-cure culture.
- HealthUnlocked · NASS communityUK patient discussion connected to NASS; useful for questions to bring back to care.
- Spondylitis Association forumModerated SAA message boards, including PT and support-group threads.
- Resistance bands + door anchorLight/medium/heavy — most AS strength work, anywhere
- Foam rollerThoracic mobility and self-myofascial release
- Yoga mat, two blocks, a strapSufficient for any home practice
- Full-length mirror + doorway pull-up barPosture checks; hanging decompression that feels miraculous
The one-page summary
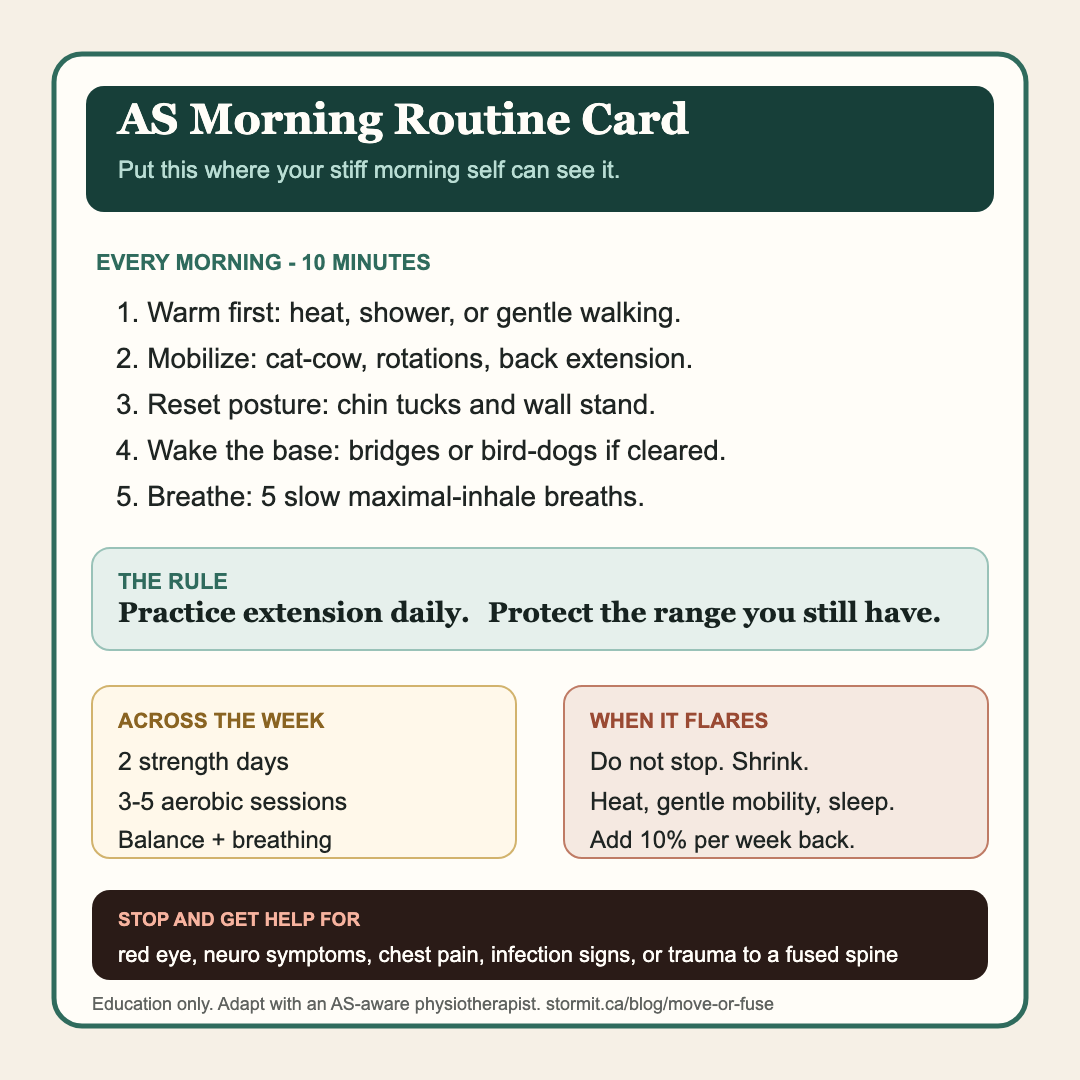
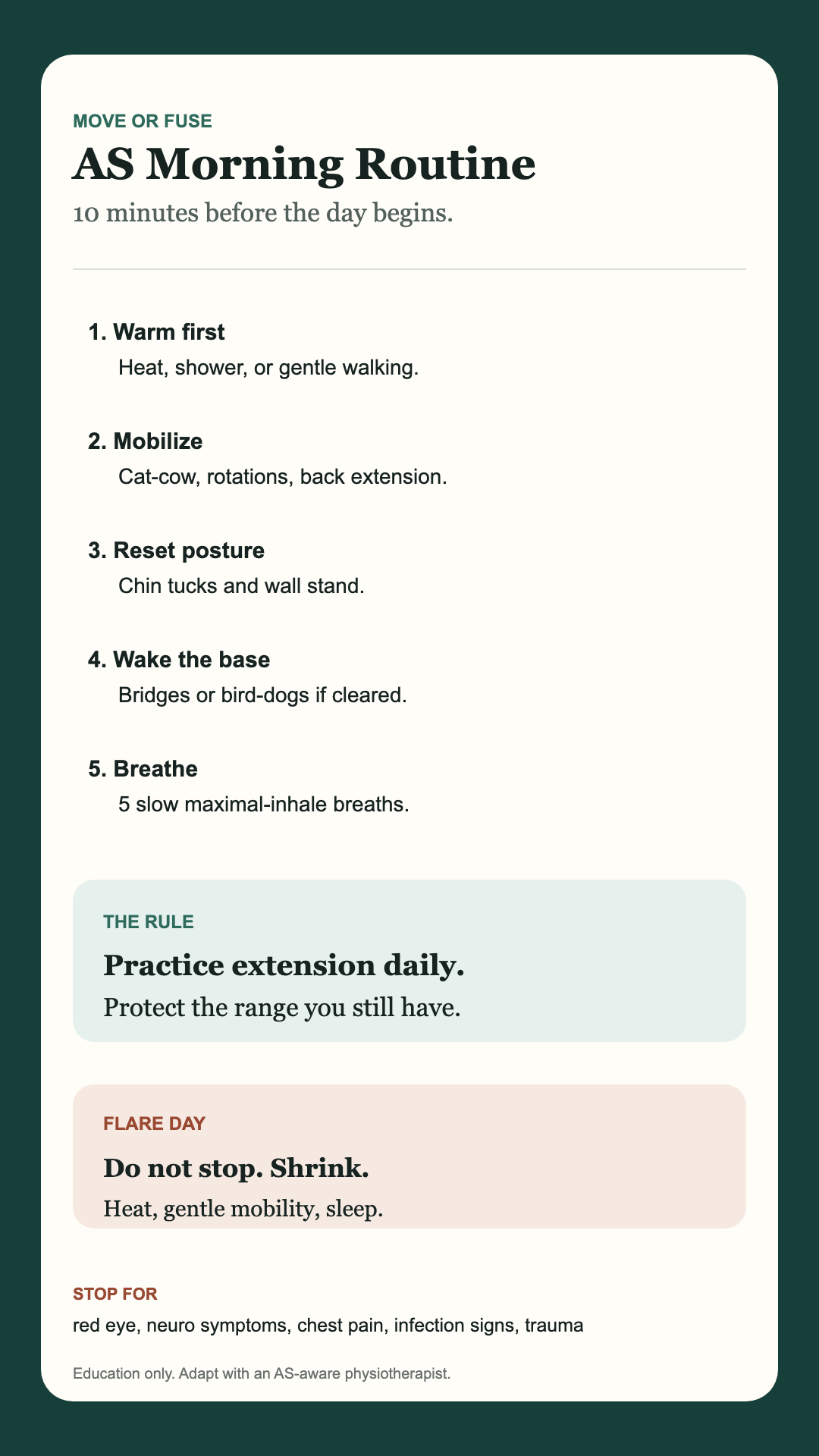
Download the AS Morning Routine Card first, then use the in-article version below as a quick reference. The point is not to admire the guide. It is to put the routine somewhere your stiff, half-awake morning self can actually see it.
Download the AS Morning Routine Card
Put it on the fridge, save it to your lock screen, share it with your AS group, or email it to yourself before the tab disappears.- Warm (hot shower / heat)
- Cat-cow, thoracic rotations, back extension
- Chin tucks + wall stand
- 5 maximal-inhale breaths
Practice extension daily. Protect the posture and range you still have.
- 2 strength days
- 3–5 aerobic sessions
- 1 aquatic / class day
- Balance + breathing
Mobility · posture · strength · aerobic · stretch · breath · balance.
Don't stop — shrink. Gentle mobility, heat, sleep, then add 10% a week back.
Red eye, new neurological symptoms, chest pain, infection on immunosuppressants, trauma to a fused spine.
Companion guide · the human side of ASThe Things You Only Learn From the AS Community→
Now go move
I'll close with the gentler version of the idea this guide keeps returning to: AS is not your fault, and movement is not a moral test. But the positions and ranges you practice most days can help protect the body you have to live in.
The drugs of the last twenty years have changed what fusion many patients experience — for some, they prevent most of it. Movement still matters because the chest you'll breathe with, the neck you'll use to look up, and the spine you'll walk with are shaped by daily inputs as well as medication. That daily practice is one piece of this disease that can remain yours — and a good physiotherapist is the partner who helps you spend it well.
Ten minutes when you wake. Thirty minutes most days. One pool session a week if you can. The seven pillars touched across the week. The choice, every single day, to move into the position you want to live in.
— small, daily, unglamorous, lifelong, and quietly heroic
References
- Levitova A, Hulejova H, Spiritovic M, Pavelka K, Senolt L, Husakova M. Clinical improvement and reduction in serum calprotectin levels after an intensive exercise programme for patients with ankylosing spondylitis and non-radiographic axial spondyloarthritis.. Arthritis Research & Therapy. 2016;18:275. DOI: 10.1186/s13075-016-1180-1. PMID: 27887637. PMCID: PMC5124318. (2016). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/27887637/
- Sveaas SH, Bilberg A, Berg IJ, Provan SA, Rollefstad S, Semb AG, Hagen KB, Johansen MW, Pedersen E, Dagfinrud H. High intensity exercise for 3 months reduces disease activity in axial spondyloarthritis (axSpA): a multicentre randomised trial of 100 patients.. British Journal of Sports Medicine. 2020;54(5):292-297. DOI: 10.1136/bjsports-2018-099943. PMID: 30745314. (2020). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/30745314/
- Kong L, Yu C, Wang C, Meng Z. Comparative efficacy of different exercise interventions in patients with ankylosing spondylitis: a systematic review and network meta-analysis.. PeerJ. 2025;13:e20336. DOI: 10.7717/peerj.20336. PMID: 41321953. PMCID: PMC12662062. (2025). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/41321953/
- Ye G, Gao L, Liu C, Huang J, Zheng X, Gao Y, Wang H, Wang H. The effectiveness of different exercise mode interventions in improving disease activity in patients with ankylosing spondylitis: a network and dose-dependent meta-analysis.. Frontiers in Physiology. 2026;16:1715944. DOI: 10.3389/fphys.2025.1715944. PMID: 41640843. PMCID: PMC12864062. (2026). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/41640843/
- Wang Y, Liu X, Wang W, Shi Y, Ji X, Hu L, Wang L, Yin Y, Xie S, Zhu J, Zhang J, Jiao W, Huang F. Adherence, efficacy, and safety of wearable technology-assisted combined home-based exercise in Chinese patients with ankylosing spondylitis: randomized pilot controlled clinical trial.. Journal of Medical Internet Research. 2022;24(1):e29703. DOI: 10.2196/29703. PMID: 35040798. PMCID: PMC8808346. (2022). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/35040798/
- Basakci Calik B, Pekesen Kurtca M, Gur Kabul E, Telli Atalay O, Taskin H, Yigit M, Tasci M, Cobankara V. Investigation of the effectiveness of aerobic exercise training in individuals with ankylosing spondylitis: randomized controlled study.. Modern Rheumatology. 2021;31(2):442-450. DOI: 10.1080/14397595.2020.1745409. PMID: 32202181. (2021). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/32202181/
- Dagfinrud H, Kvien TK, Hagen KB. Physiotherapy interventions for ankylosing spondylitis.. Cochrane Database of Systematic Reviews. 2008;(1):CD002822. DOI: 10.1002/14651858.CD002822.pub3. (2008). Accessed: Jul. 9, 2026. [Online]. Available: https://doi.org/10.1002/14651858.CD002822.pub3
- Ramiro S, Nikiphorou E, Sepriano A, Ortolan A, Webers C, Baraliakos X, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update.. Annals of the Rheumatic Diseases. 2023;82(1):19-34. DOI: 10.1136/ard-2022-223296. PMID: 36270658. (2023). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/36270658/
- Roşu MO, Ţopa I, Chirieac R, Ancuta C. Effects of Pilates, McKenzie and Heckscher training on disease activity, spinal motility and pulmonary function in patients with ankylosing spondylitis: a randomized controlled trial.. Rheumatology International. 2014;34(3):367-372. DOI: 10.1007/s00296-013-2869-y. PMID: 24071935. (2014). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/24071935/
- Schieir O, Tosevski C, Glazier RH, Hogg-Johnson S, Badley EM. Incident myocardial infarction associated with major types of arthritis in the general population: a systematic review and meta-analysis.. Annals of the Rheumatic Diseases. 2017;76(8):1396-1404. DOI: 10.1136/annrheumdis-2016-210275. PMID: 28219882. (2017). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/28219882/
- Zhao S, Thong D, Miller N, Duffield SJ, Hughes DM, Chadwick L, Goodson NJ. The prevalence of depression in axial spondyloarthritis and its association with disease activity: a systematic review and meta-analysis.. Arthritis Research & Therapy. 2018;20:140. DOI: 10.1186/s13075-018-1644-6. PMID: 29996916. PMCID: PMC6042424. (2018). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/29996916/
- Lane B, McCullagh R, Cardoso JR, McVeigh JG. The effectiveness of group and home-based exercise on psychological status in people with ankylosing spondylitis: a systematic review and meta-analysis.. Musculoskeletal Care. 2022;20(4):758-771. DOI: 10.1002/msc.1641. PMID: 35437893. (2022). Accessed: Jul. 9, 2026. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/35437893/
- National Axial Spondyloarthritis Society (NASS). Exercise, Back to Action, hydrotherapy, and physiotherapy resources.. nass.co.uk. (accessed 2026). Accessed: Jul. 9, 2026. [Online]. Available: https://www.nass.co.uk/
- Spondylitis Association of America. Exercise resources and patient education for spondyloarthritis.. spondylitis.org. (accessed 2026). Accessed: Jul. 9, 2026. [Online]. Available: https://spondylitis.org/
- Canadian Spondyloarthritis Association. Patient resources and Canadian support for spondyloarthritis.. spondylitis.ca. (accessed 2026). Accessed: Jul. 9, 2026. [Online]. Available: https://spondylitis.ca/


{kind=link}
{kind=link}